
A corpus callosotomy is a surgical procedure for severe, drug-resistant epilepsy that involves cutting the nerve fibres of the corpus callosum, the thick band connecting the brain’s two hemispheres. By severing this bridge, the procedure stops seizure signals from spreading from one side of the brain to the other, which prevents the generalised electrical storms that cause dangerous drop seizures. The surgery does not remove brain tissue and works as a palliative option when antiepileptic drugs fail to control atonic or tonic falls.
According to Dr. Gurneet Singh Sawhney, a respected neurosurgeon in Mumbai, Drop seizures don’t respond to medication in many patients, and even one fall can cause skull fractures. Disconnecting the callosum stops the seizure from generalising, so the body doesn’t lose tone on both sides at once.
Falls during seizures leaving bruises or injuries every week?
Why does the corpus callosum cause drop seizures?
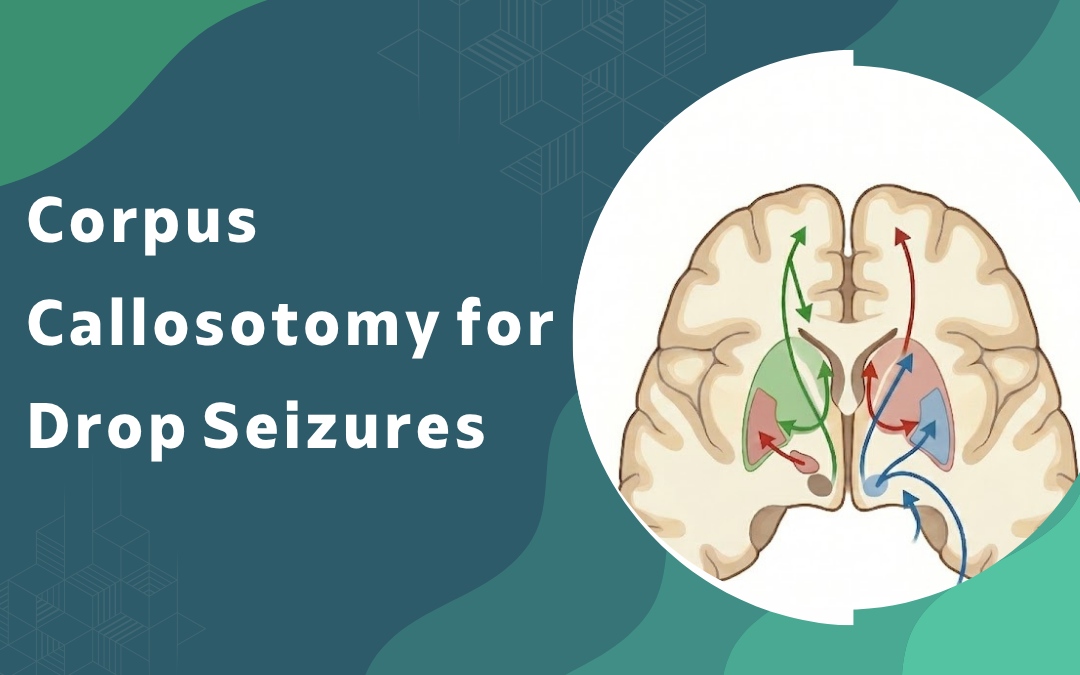
The corpus callosum acts like a high-speed bridge between the two halves of the brain. When epileptic activity crosses it unchecked, both sides lose control together and the body collapses without warning.
- Signal highway: Abnormal discharges starting on one side travel through the callosum within milliseconds, recruiting the opposite hemisphere and triggering a generalised electrical storm across both sides.
- Tone loss: Atonic seizures cut muscle tone on both sides simultaneously, which is why patients drop straight down without bracing or any protective reflex.
- Tonic stiffening: In tonic drop attacks the body goes rigid first, then falls. Same mechanism, opposite muscle response.
- Refractory pattern: When two or more antiepileptic drugs fail, the spread pattern itself becomes the problem. And that’s where surgery enters.
So the target isn’t the seizure focus. It’s the road the seizure travels on. Cut the road, and the attack stays on one side. Read more about epilepsy surgery options before consulting.
How does the surgery actually stop the falls?
The neurosurgeon disconnects either the front two-thirds or the entire callosum, depending on seizure type and patient age. Microsurgical technique under neuronavigation keeps surrounding structures untouched.
- Anterior section: First-line approach for most adults, cutting roughly two-thirds of the callosum and preserving the splenum to limit cognitive side effects.
- Total callosotomy: Used when anterior surgery doesn’t reduce drop attacks enough, or in severe paediatric cases linked to brain tumour treatment and cortical malformations.
- Recovery: Hospital stay runs five to seven days, and most patients return to routine activity inside four to six weeks.
- Outcome: Roughly 70 per cent of patients see major reduction in falls, sometimes complete cessation of drop attacks.
But the surgery is palliative. Other seizure types may continue, just without the dangerous falls. For more on related procedures, see awake brain surgery.
Why Choose Dr. Gurneet Singh Sawhney?
Dr. Gurneet Singh Sawhney is a senior consultant neurosurgeon and spine specialist with over 18 years of experience in complex brain and epilepsy surgery. His training includes advanced fellowships in functional neurosurgery and minimally invasive techniques.
Patients with drug-resistant epilepsy come to him after years of failed medication trials. The clinic handles surgical workup, intraoperative monitoring, and long-term seizure follow-up under one roof. No referral chains, no delays.
FAQ's
Is corpus callosotomy a permanent procedure?
Yes, the disconnection is permanent and the callosum does not regrow.
Can the surgery cure epilepsy completely?
No, it stops drop seizures but other seizure types may persist after surgery.
How long is the recovery period?
Most patients resume daily routine within four to six weeks post-surgery.
Is the surgery suitable for children?
Yes, it is often more effective in children with severe refractory drop attacks.