
Trigeminal neuralgia is a persistent pain that affects the trigeminal nerve, which sends sensations from the facial area to the brain. If you have trigeminal neuralgia, even minor facial stimulation, such as brushing the teeth or applying cosmetics, can cause terrible pain.
You may have brief and moderate bouts at first. However, trigeminal neuralgia can worsen over time, resulting in longer and more frequent episodes of shooting pain. Trigeminal neuralgia is more common in women than in males, and it is more common in those over 50.
Any physical contact with the face can set off an episode. It is one of the most distressing disorders, and it can lead to depression. The leading cause for this is unknown.
The patient must first identify a trigger before seeking treatment from a competent neurosurgeon to get the best results from trigeminal neuralgia treatment. Dr. Gurneet Singh Sawhney, one of the top neurosurgeons in Mumbai, has expertise in treating trigeminal neuralgia through medical and surgical interventions.
Symptoms of Trigeminal Neuralgia
- Severe shooting or jabbing pain seems like an electric shock at times.
- Pain attacks occur without warning or are provoked by touching the face, speaking, chewing, or brushing one’s teeth.
- Pain bursts that range anywhere from a few seconds to several minutes.
- Multiple attacks that last days, weeks, months, or longer. Some people go through periods where they are pain-free.
- A persistent aching, burning sensation may start before trigeminal neuralgia progresses to spasm-like pain.
- The trigeminal nerve transmits pain to the teeth, cheek, jaw, gums, lips, and, less commonly, the eye and forehead.
- The pain usually affects only one side of the face at a time, though it can occasionally impact both.
- Pain can be localized or radiate out over a larger area.
- Over time, attacks become more regular and intense.
How is trigeminal neuralgia diagnosed?
There are a variety of causes for facial pain. Frequently, migraine, post-herpetic neuralgia, cluster headache, and temporomandibular joint disease are misdiagnosed as trigeminal neuralgia.
A neurologist or neurosurgeon classifies the pain based on facial discomfort’s nature, location, and triggers to confirm trigeminal neuralgia. To identify whether trigeminal neuralgia is caused by neurovascular conflict, multiple sclerosis, or a tumour, reflex tests and a neurological examination with an MRI are required.
Treatments for Trigeminal Neuralgia
Medical treatment :
Carbamazepine is the most commonly prescribed medication. To control pain, the therapeutic idea is to use the smallest single dose possible. The frequency is changed until the pain is completely gone. Once sustained remission is obtained, the regimen is maintained for another 6-8 weeks without changing the dose.
After that, the medicine can be progressively reduced and discontinued. This can be restarted in the event of a recurrence of pain. Recurrences are less responsive with time, necessitating the use of different medications.
Surgical treatment :
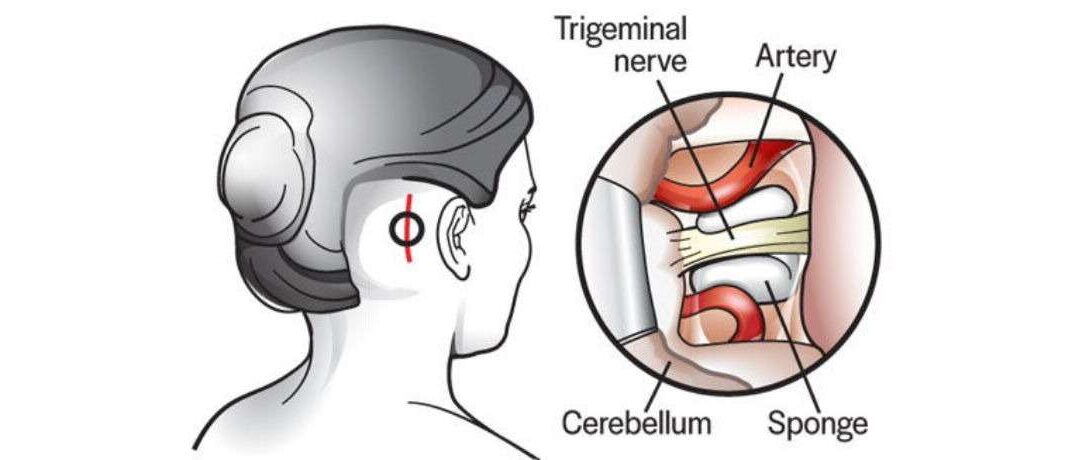
Microvascular decompression (MVD) and radiofrequency thermocoagulation (RFTC) are the two most popular surgical procedures. Microvascular decompression (MVD) is a procedure that includes exploring the posterior fossa through a small hole adjacent to the mastoid process. The problematic vascular loop is dissected free of the root entrance zone under magnification, and a Teflon graft is placed.
Radiofrequency Thermocoagulation :
The temperature-dependent selective destruction of the pain-transmitting C fibres while preserving the A-delta fibres is the basis of radiofrequency rhizotomy. This is a procedure used in daycare.
The preoperative workup includes a physical examination to determine whether or not you are fit to endure general anaesthesia for a short period. Percutaneous retrogasserian needle implantation is used in this procedure.

Radiofrequency ablation is a minimally invasive, safe, and successful method for treating drug-resistant trigeminal neuralgia. The results are similar to those obtained with microvascular decompression.
Rf ablation has been the procedure of choice in recent years, particularly for elderly patients and those with a high risk of anaesthetic complications. Using radiofrequency electrical stimulation, this treatment selectively kills nerve fibres associated with pain.
A neurosurgeon administers anaesthesia to insert and guide a hollow needle into the trigeminal nerve. Then, the patient is brought out of sedation. A mild signal is applied after an electrode is passed through the needle to confirm the pain site.
The patient has anaesthetized again for radiofrequency thermal lesioning after the target nerve fibre is confirmed. The neurosurgeon selectively heats the nerve fibre by heating the electrode until it is damaged and a lesion area forms. After the surgery, the patient may have face numbness for a few hours.
Microvascular decompression :

Microvascular decompression is a procedure that includes isolating blood vessels that are squeezing the trigeminal nerve. The damaged trigeminal nerve is either relocated or removed from contact with the blood vessel.
On the side of pain, the neurosurgeon makes a cut behind the ear. Then, the surgeon punctures the skull with a small hole and moves the arteries along the trigeminal nerve. The area between the nerve and the arteries is cushioned.
The majority of the time, microvascular decompression is successful. In rare situations, though, the pain may return. In contrast to radiofrequency ablation, patients do not feel facial numbness. However, there is a risk of hearing loss, facial paralysis, stroke, or other consequences.
Stereotactic radiosurgery:

Stereotactic radiosurgery is a type of non-invasive radiation that has a high rate of success. The neurosurgeon utilizes a highly focused radiation beam to destroy the target trigeminal nerve fibre in this surgery. After a few weeks following radiosurgery, pain alleviation becomes apparent. The surgery may be repeated if the pain returns.
The patient has the last say on whether or not to pursue treatment. However, it should not be the case that the person is unaware that he can be cured. Please be mindful of the situation. Doctors are pleading with the public to assist them in diagnosing and treating this condition.